
From the Department of Physical Medicine and Rehabilitation, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, Kaohsiung, Taiwan
#These authors contributed equally to this article.
Objective: To compare the outcomes of ultrasound-guided vs direct approach corticosteroid injection in patients with idiopathic carpal tunnel syndrome.
Methods: A double-blind randomized controlled study. Wrists affected by carpal tunnel syndrome were randomized to the ultrasound-guided (n = 22 wrists) or direct approach injection group (n = 17 wrists) before receiving 1 ml Betamethasone. Outcome measures were physical findings and electrodiagnostic parameters assessed at 1, 3 and 6 months after injection. Complications were also recorded.
Results: Both groups showed improvement through-out the follow-up period after injections, in physical findings and in most electrodiagnostic parameters (all p<0.05). The ultrasound-guided injection group showed greater improvements in the Semmes-Weinstein Monofilament test result (p = 0.004), sensory nerve conduction velocity (p = 0.038), and digit-4 comparison study result (p = 0.046). Three wrists with weakness were found in the direct approach injection group, yet none were noted in the ultrasound-guided injection group (p=0.040).
Conclusion: Both ultrasound-guided and direct approach corticosteroid injection protocols improved clinical symptoms and signs, physical function, and most electrodiagnostic parameters of patients with carpal tunnel syndrome throughout the follow-up period. However, the ultrasound-guided injection group showed greater improvements in the Semmes-Weinstein Monofilament test, sensory nerve conduction velocity, and digit-4 comparison study.
Key words: carpal tunnel syndrome; sonography; corticosteroid; injection.
Accepted Nov 17, 2017; Epub ahead of print Jan 22, 2018
J Rehabil Med 2018; 50: 200–208
Correspondence address: Ya-Ping Pong, Department of Physical Medicine and Rehabilitation, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of Medicine, No. 123, Ta-Pei Road, Niao-Sung District, Kaohsiung 83305, Taiwan. E-mail: yaping0707@gmail.com
Carpal tunnel syndrome (CTS) is a median nerve neuropathy at the wrist caused by compression of the flexor retinaculum (1). Compression of the median nerve leads to nerve ischaemia, impairment of neural conduction, and nerve damage (2). Most cases are idiopathic, but CTS can also be caused by trauma, vascular lesions, inflammation, obesity, occupational exposure, older age, osteoarthritis, pregnancy, hypothyroidism, or autoimmune diseases (3–6). Burning, tingling, and paraesthesia in the distribution of the median nerve distal to the wrist are common symptoms of CTS (4, 6). Electrodiagnostic tests can help confirm the diagnosis of CTS (7). Treatments for CTS include splinting, oral corticosteroids, non-steroidal anti-inflammatory drugs, or botulinum toxin injections (8–11). The preferred treatment for neurophysiologically verified CTS with severe symptoms is surgical decompression. Research into the efficacy of treatment is ongoing, but the results are variable due to the fact that studies differ with respect to design, severity of CTS, medication types and doses, and follow-up periods.
Local corticosteroid injection is considered in most mild to moderate cases of CTS (7), and a number of randomized controlled trials have documented treatment efficacy. In one systematic meta-analysis (12), local corticosteroid injection for CTS significantly improved clinical symptoms 1 month after injection compared with placebo. Local corticosteroid injection also contributed to greater clinical improvement vs oral corticosteroid for up to 3 months, but no long-term clinical benefit was evaluated. In addition, there have been some reports regarding median nerve injury from local steroid injection in CTS (13–15).
Sonography examinations are fast, convenient, and non-invasive. Because of technical advances in high-resolution sonography, clinicians have begun to guide therapeutic carpal tunnel injections by sonography in appropriately selected patients (16, 17). Ultrasound-guided injections have proven to result in better outcomes in 2 randomized controlled trials (18, 19). In one network meta-analysis (20), ultrasound-guided injections provided greater clinical benefits than direct injections. In these studies, however, patients were followed up for only 3 months and the studies were not blinded, therefore making it difficult to exclude the possibility that the results may have been biased. The aim of this study was to compare the long-term (up to 6 months) outcomes of ultrasound-guided corticosteroid injection with direct approach injection in patients with CTS.
This was a double-blind randomized controlled trial comparing the effectiveness of ultrasound-guided vs direct approach injections of 1 ml Betamethasone (Bufencon®, Yungshin Pharm Ind. Co. LTD, Taiwan) in patients with idiopathic CTS.
Forty consecutive patients with 52 wrists with a clinical and neurophysiological diagnosis of idiopathic CTS were recruited between September 2011 and January 2014 from a single medical centre. Inclusion criteria were: (i) age between 18 and 80 years; (ii) ≥ 2 of the following symptoms: nocturnal paraesthesia; symptomatic relief after shaking hands; pain or paraesthesia when hand gripping; or sensory symptoms over thumb, index, middle, or part of ring fingers; (iii) symptom duration ≥ 1 month; (iv) mild to moderate CTS, defined as slowing of the sensory conduction velocity or abnormal distal motor latency according to a validated CTS electrophysiological severity scale (21).
Exclusion criteria were: (i) symptomatic CTS because of diabetes, thyroid disease, or chronic kidney disease; (ii) absence of median motor and sensory response in electrodiagnostic tests; (iii) muscle atrophy of abductor pollicis brevis; (iv) traumatic nerve injury; (v) peripheral polyneuropathy; (vi) previous surgery or local corticosteroid injection of the affected wrists; (vii) pregnancy; (viii) cognitive impairment or other psychiatric disorders; and (ix) inability to complete 6-month follow-up.
The study protocol was approved by Chang Gung Medical Foundation Institutional Review Board (IRB number: 99-4155A3) and was registered at ClinicalTrials.gov (Clinical Trial Identifier NCT02575729). The study was conducted in accordance with the ethical standards on human experimentation and with the principles of the Declaration of Helsinki 1975, revised in 1983. All participants provided signed informed consent prior to enrolment.
Patients were randomly assigned to a sonography approach (ultrasound-guided) injection group (SAG, n = 30 wrists) or direct approach injection group (DAG, n = 22 wrists) by use of a coin toss. All allocations were concealed in opaque envelopes. The research assistant enrolled the participants, generated the allocation sequence, and assigned participants to their groups. Betamethasone 1 ml (Betamethasone 1 ml /amp, 1 ml contains betamethasone dipropionate 5 mg and betamethasone disodium phosphate 2 mg) was injected into the ulnar side of the palmaris longus tendon. Other therapies, such as medications, splinting, or complementary treatments, were not allowed during the 6-month follow-up period.
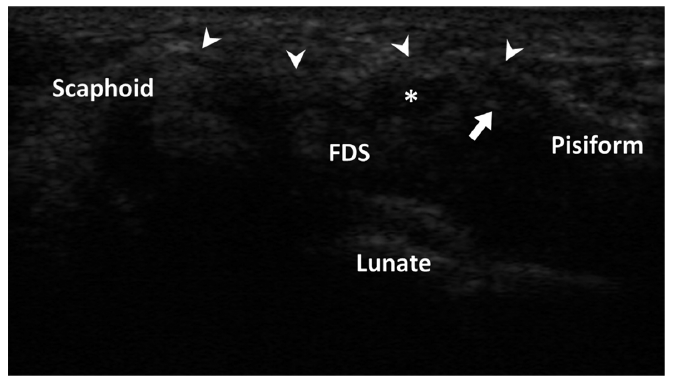
Two experienced physicians performed the injections. In the SAG, the procedure was performed using a sonography device (t3000, Terason, Burlington, VT, USA). The patients were asked to maintain a seated position facing the physician, with their wrists resting in a supinated position on the table. The out-plane approach was used for the ultrasound-guided injection technique, in which the transducer was placed perpendicular to the median nerve. The pisiform bone, scaphoid bone, median nerve, flexor retinaculum, and flexor digitorum superficialis tendon were brought into view (Fig. 1). After sterilization of the skin, a 27-gauge needle was inserted into the proximal carpal tunnel at the distal wrist crease and ulnar to the area adjacent to the median nerve (19, 22). The physician performed the injection by inserting the needle through the flexor retinaculum, avoiding harm to the median nerve, ulnar nerve and artery, and flexor digitorum superficialis tendon. The tip of the needle was identified as a moving reflector in real time as the tip passed obliquely from the skin surface of the proximal carpal tunnel (18). In the DAG, the patients were also asked to maintain the same posture. The needle was also inserted to the proximal carpal tunnel at the distal wrist crease just ulnar to the palmaris longus tendon after sterilization of the skin. Sham ultrasound guidance was used to maintain participant blinding.
Fig. 1. Transverse sonogram of the proximal carpal tunnel. *Median nerve; arrow: needle tip; arrowhead: flexor retinaculum. FDS: flexor digitorum superficialis.
The physical findings were measured at baseline, 1, 3, and 6 months after the injections by a research assistant blinded to the patient allocation. The electrophysiological findings were also evaluated at the same time-points by a physician blinded to the patient allocation. The physician had been well trained in electrodiagnosis.
For physical findings, CTS-related symptoms and signs, such as hand weakness, constant numbness, daytime numbness, Tinel’s sign, Flick sign, Phalen’s test, Reverse Phalen’s test, and wrist compression test, were recorded. For light touch pressure, the Semmes-Weinstein Monofilament test (SWMT) was conducted on the index fingers to test light touch pressure sensation (23, 24). Twenty different monofilaments were used, with sizes ranging from 1.65 to 6.65. The size 2.83 represents normal light touch function, and increasing size of monofilaments is indicative of worsening function. These outcome measures were transformed into 20 ranks. Grip strength and lateral pinch strength were measured using a Jamar dynamometer (Sammons Preston. Rolyan, Bolingbrook, IL, USA) in the position standardized by American Society of Hand Therapists (25). The mean score of 3 trials was recorded for each hand (26). A validated questionnaire, Boston Carpal tunnel Questionnaire (BCTQ), is most commonly used to evaluate the improvements in symptom severity and functional status of patients with CTS (27). This questionnaire consists of 2 parts; the first part (11 items) assesses symptom severity of the hand (symptom severity scale (SSS)) and the second part (8 items) assesses functional status of the hand (functional status scale (FSS)). Each question has 5 answers, which are scored 1–5 according to symptom severity or functional difficulty. A higher score indicates more severe symptoms or poorer function (27). The 100-mm visual analogue scale (VAS) was used to subjectively quantify the overall disease severity (28), ranging from 0 (normal condition) to 100 (worst condition).
Electrophysiological findings were measured using a Nicolet Viking Quest electromyography machine (Nicolet Biomedical Inc., Madison, WI, USA) to record distal motor latency (DML) and compound motor action potential (CMAP) at the abductor pollicis brevis muscle. The sensory distal latency (SDL, including peak and onset latency), sensory nerve conduction velocity (SNCV) across the wrist, and sensory nerve action potential (SNAP) were stimulated at the wrist and assessed at the index finger. The digit-4 comparison study (Digit4) was evaluated at the ring finger to calculate the median-to-ulnar sensory nerve distal latency difference.
According to the study by Ustün et al. (19), ultrasound-guided injection was more effective than the direct approach injection when outcomes were assessed using the BCTQ symptom severity. The sample size calculation for the BCTQ symptom severity scale was based on a 2-sample t-test. In this clinical trial, the mean difference and standard deviation after treatment for 12 weeks were –1.3 and 0.58 in the SAG, and –0.69 and 0.70 in the DAG, respectively. We set these conditions at a 2-sided significance level of 0.05 with a power of 0.80, and it was determined that the study required at least 38 subjects. With an estimated dropout rate of 20%, we calculated that the total number of enrolled subjects should be 48.
Statistical analyses were conducted using the software Stata (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP). The baseline characteristics of patients were calculated with descriptive statistics. Per-protocol analysis was conducted to evaluate the treatment effect. The changes from baseline to 1, 3, and 6 months for each outcome measure were computed using the generalized estimating equation (GEE) for repeated measures. GEE modelling was based on linear function and AR-1 correlation structure. The level of statistical significance was set at p < 0.05.
Forty patients with 52 wrists with CTS were enrolled in this study. Baseline characteristics, including age, body mass index, repetitive manual work, symptom duration, SWMT, CMAP, SNCV, and SNAP are described in Table I. The SAG included 30 wrists, and the DAG included 22 wrists with CTS. After treatment for 6 months, 8 wrists (26.7%) were lost to follow-up in the SAG and 5 wrists (22.7%) were lost to follow-up in the DAG due to treatment failure or surgical referral. Therefore, at the time of study completion, we analysed the results of 22 wrists in the SAG and 17 wrists in the DAG (Fig. 2).
Table I. Patient characteristics stratified by injection groups
Fig. 2. Patients’ flow diagram. SAG: sonography approach (ultrasound-guided) injection group; DAG: direct approach injection group.
Binary outcomes. At all 3 time intervals after injection, both the SAG and the DAG showed significant improvement in most of the outcomes, including hand weakness, constant numbness, daytime numbness, Tinel’s sign, Flick sign, Phalen’s test, Reverse Phalen’s test, and wrist compression test (Table SI1). The effects were most prominent at 1 month and 3 months after the injection. Although the main effect of time was significant for each outcome, the interaction effect of time and group and the main effect of group were not (Table II).
Table II. Physical findings of the patients, binary outcome
Numerical outcomes. Significant improvement in SWMT, SSS, FSS and VAS were demonstrated in both the SAG and the DAG over time. Significant improvement in grip strength was found only in the SAG group at 1 month, but not at subsequent time-points, and was not found in the DAG group (Table SII1). The main effect of time was significant for all outcomes, but the main effect of group and the interaction effect of time and group were significant only in SWMT (p = 0.031 and p = 0.004, respectively) (Table III).
Table III. Physical findings of the patients, numerical outcome
DML, SDL (onset), and Digit4 presented significant improvements at 1 and 3 months after the injection, while SDL (peak) only showed significant improvement at 3 months after the injection in both groups. However, there was significant improvement in SNCV at 1 and 3 months, CMAP at 3 month and DML at 6 months after the injection only in the SAG. Compared with the DAG, SAG had significant improvement in SDL (onset) and SNCV at 3 months (Table SIII1). With respect to the main effect of time, all of the outcomes showed significance except for CMAP and SNAP (p = 0.065 p = 0.111, respectively). The interaction effect of time and group was significant in SNCV and Digit4 (p = 0.038 and p = 0.046, respectively) (Table IV).
Table IV. Patients’ electrophysiological findings
The discomforts experienced by patients within the first week after local injections are reported in Table V. Numbness after injections was observed in 1 wrist in the SAG and 4 wrists in the DAG. A sensation of swelling was noted in 4 wrists in the SAG and 6 wrists in the DAG. Pain after injections occurred in 10 wrists in both groups. Three patients in the DAG felt wrist flexor or extensor weakness, but none were noted in the SAG (p = 0.040). All these complications were temporary and none of the patients had persistent symptoms at follow-up visits.
Table V. Patient discomfort within one week after local injection (n = 39)
This study analysed 39 wrists with idiopathic CTS receiving local corticosteroid injections through ultrasound-guided or direct approach, with follow-up at 1, 3, and 6 months after the treatments. Twenty-two wrists received ultrasound-guided local corticosteroid injections and 17 wrists received local corticosteroid injections through the direct approach. Physical findings with binary outcomes, including hand weakness, constant numbness, daytime numbness, Tinel’s sign, Flick sign, Phalen’s test, Reverse Phalen’s test, and wrist compression test, improved significantly at 1, 3, and 6 months after the treatment in both groups, with no significant differences noted between groups. For numerical outcomes, SWMT, SSS, FSS, and VAS demonstrated significant improvements over time in both groups. However, the SAG showed significantly more improvement in SWMT than the DAG (p = 0.004). The electrophysiological findings DML, SDL (onset), and Digit4 improved significantly at 1 and 3 months after the treatments in both groups, but SNCV showed significant improvement at 1 and 3 months after the treatments only in the SAG. Compared with the DAG, the SAG was more efficient at improving SNCV and Digit4 (p = 0.038 and p = 0.046, respectively).
The clinical benefits of local corticosteroid injections for patients with CTS have been outlined in 1 meta-analysis (12). Ultrasound-guided injections provided greater clinical benefits than direct injections in 1 recently published network meta-analysis (20). Among the included randomized controlled trials (18, 19) of this network meta-analysis, SSS, FSS, and electrophysiological findings were reported. Our study reported not only the above findings, but also results of physical and clinical examinations (SWMT, grip and lateral pinch strength). Ustün et al. (19) demonstrated in one single-blind clinical trial that the ultrasound-guided injection group showed greater improvements in SSS than the direct injection group at 12-week follow-up, but no difference was observed in our study. Since SSS was a subjective indicator, this variable would be more reliable if obtained from a double-blind study design. In the study by Lee et al. (18), there was no significant difference in SSS between the out-plane ultrasound-guided injection and direct injection groups, consistent with our own results. CMAP, SNAP, and SDL were improved in the ultrasound-guided injection group, but only SNAP was improved in the direct injection group. Eslamian et al. (29) found that SSS, FSS, and 4 electrodiagnostic parameters (DML, SDL, SNAP, SNCV) were all significantly improved in both the ultrasound-guided (in-plane injection) and direct injection groups at 12-week follow-up. In our study, we also found that most electrodiagnostic parameters (DML, SDL, Digit4) were improved at 12-week follow-up in both groups, but CMAP and SNCV were significantly improved only in the ultrasound-guided injection group. Significant differences between the 2 groups at 12-week follow-up were only found with SDL (onset) and SNCV, but not with SSS, FSS, or other electrodiagnostic parameters. The difference in results between our study and the above-mentioned studies may be due to differences in study design (single-blind or double-blind), injections (different types of corticosteroid preparations with or without lidocaine), inclusion criteria for participants, or even specialists’ experience in ultrasound-guided and direct injection. Unlike the previous studies (19, 20, 29), we used sham ultrasound guidance so that patients remained blind to their allocations throughout the study. This procedure may improve the reliability of subjective outcome measures, such as SSS and FSS. In addition, the above studies (18, 19, 29) only reported outcomes up to 12 weeks of follow-up, whereas we reported outcomes up to 6 months of follow-up. At 6-month follow-up, we found no significant difference between the 2 groups in all parameters, but significant improvements of SWMT, SSS, and VAS occurred in both groups, with improvements in DML in only the SAG group. Although Makhlouf et al. (30) also compared the outcomes of these 2 injection techniques at 6-month follow-up, the results lacked objective findings (only procedural pain, pain scores, and responder rates were reported). In a recent community-based cohort study, Evers et al. (31) found that ultrasound-guided injection was associated with a reduced hazard of retreatment, but the research was also short of objective outcomes.
For direct steroid injection in CTS, there is no consensus regarding the optimal local corticosteroid injection sites for CTS. The usual injection site for the proximal injection approach is the proximal carpal tunnel near the flexor crease and just ulnar to the palmaris longus tendon. If patients have no palmaris longus tendon, then an alternative approach is ulnar to the midline of the wrist or just ulnar to the flexor carpi radialis tendon (32–35). Habib et al. (36) proposed a distal injection approach, in which the injection site was 2–3 cm distal to the flexor crease. The authors did not find any significant difference in clinical outcomes between the proximal and distal injection groups, but the operating time was shorter in the distal injection group. The distal injection approach was considered safer than the proximal injection approach because the former injection site can avoid damage to the flexor tendons, median nerve and blood vessels in the carpal tunnel (36). However, the median nerve was still visible in the superficial layer of the palm during ultrasound examination when the probe was placed on the site distal to the flexor crease, and therefore susceptible to damage. There are risks for median nerve injury if the injections are performed within 1 cm on either the ulnar or the radial side of the palmaris longus tendon (37), and several reports of median nerve injury have been published (13–15). No median nerve or tendon injury was found in this study. In 2 recent randomized controlled trials (18, 19), the complications were reported with varying degrees. Ustün et al. (19) did not observe any major side-effects except for procedural pain. However, Lee et al. (18) described 3 categories of post-treatment complications (nerve insult, vessel insult, and skin lesion). In the present study, complications within 1 week after local injections were recorded as numbness, sensation of swelling, pain, and weakness. Three patients felt weakness after local injections in the DAG, but no weakness was observed after injections in the SAG (p < 0.04). Decreased amplitude of SNAP at 1 month after injections with later recovery was observed. Mild axonal injury was probably due to direct trauma during blind injection, but the recovery of the nerve was relatively good.
Ultrasound guidance has advantages of low cost, convenience, and accuracy. The real-time capability of sonography enables physicians to visualize the needle tip throughout the entire duration of the procedure and to avoid accidental injury to the nerve and surrounding structures (38, 39). In addition, ultrasound can help physicians to more accurately guide the medication to the target site and visualize whether the distribution of injected corticosteroid is adequate (38, 40). The physician may keep the needle closer to the median nerve under ultrasound guidance to increase the medication effect and promote better improvement. However, we could not confirm whether medication was around the median nerve with direct injection technique. Because median nerve is quite shallow at the wrist, we may preform blind injection with a smaller angle to the skin to prevent needle injury to the median nerve. We may also stop the insertion and change the insertion direction when patients felt pain or numbness. The above-mentioned direct injection procedure cannot confirm whether the medication gets into the carpal tunnel and around the median nerve.
This study had several limitations. Firstly, the majority of patients in both groups were female. The sex disparity in CTS rates in our study was similar to that reported previously (41). Secondly, the reported discomforts within 1 week after injections for CTS in the present study were different from the complications or discomforts described in other studies (18, 19). This discrepancy could be avoided in the future by developing a standardized method for reporting CTS injection complications (42–44). Thirdly, the dropout rates of both groups in our study were higher than the accepted values in other randomized controlled trials. The only reasons for loss to follow-up were treatment failure or surgical referral. Nevertheless, the number of subjects who completed the study was sufficient for final statistical analysis according to the sample size estimation. Fourthly, the BMI in DAG was higher than that in SAG. Although no significant difference was found (p = 0.072), we could not exclude the influence of BMI on the outcome of steroid injection. Fifthly, some self-evaluated outcomes, such as SSS, FSS, or VAS, could be biased if both wrists of 1 patient were included. Finally, all enrolled subjects were from one tertiary medical centre in southern Taiwan, which might lead to some selection bias.
Both the ultrasound-guided injection and the direct approach injection were effective in improving clinical symptoms, signs, function, and most electrophysiological findings in patients with CTS at 1, 3, and 6 months follow-up. However, the ultrasound-guided injection group showed greater improvement in SWMT, SNCV, and Digit4 throughout follow-up. A confirmation of the clinical benefits of SAG was obviously not achieved for SSS. This could be because earlier studies have exaggerated the effects and/or the power of this study was too low.
This study was supported by a grant from the National Medical Research Program, Taiwan (NMRPG8A0051).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize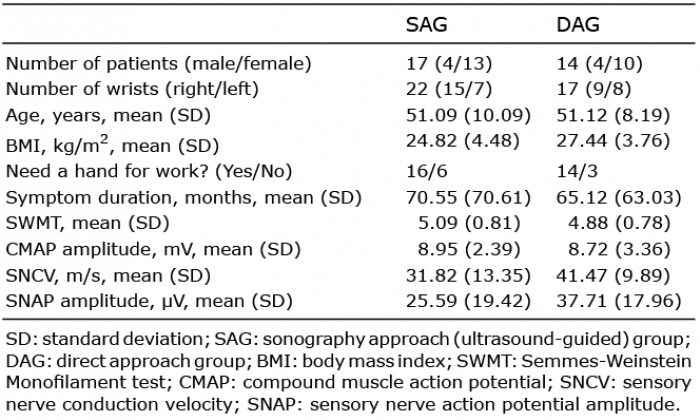 Click to show fullsize
Click to show fullsize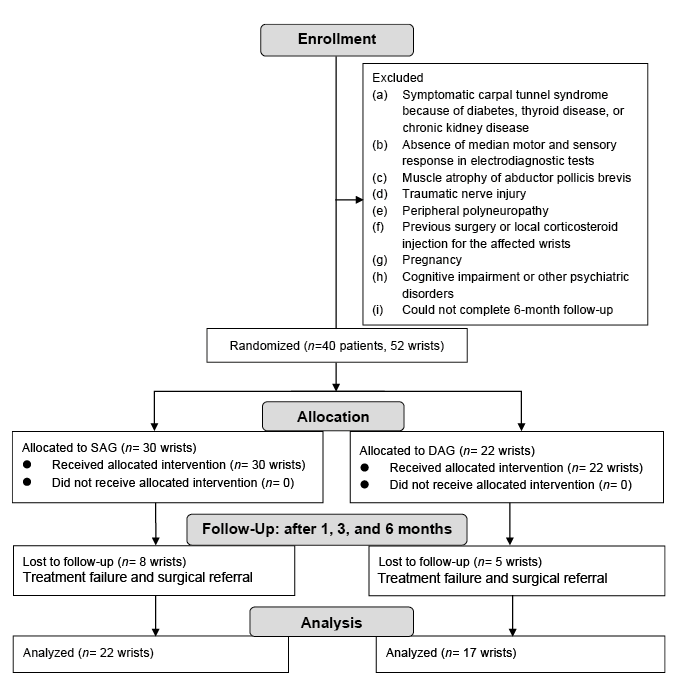 Click to show fullsize
Click to show fullsize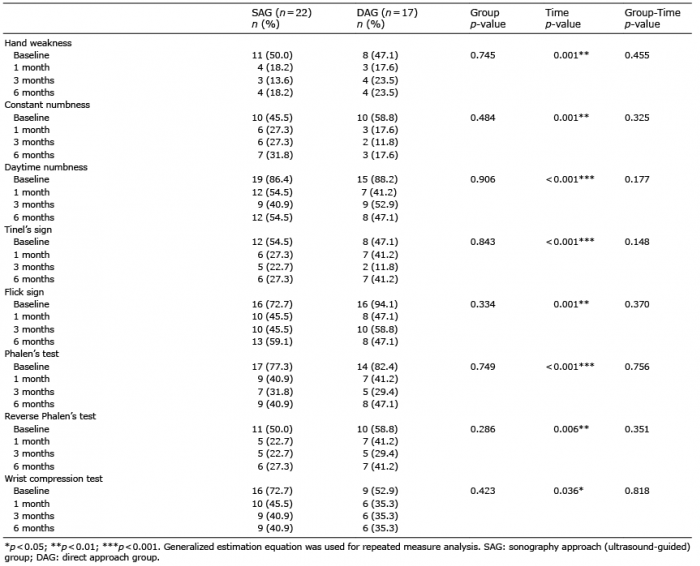 Click to show fullsize
Click to show fullsize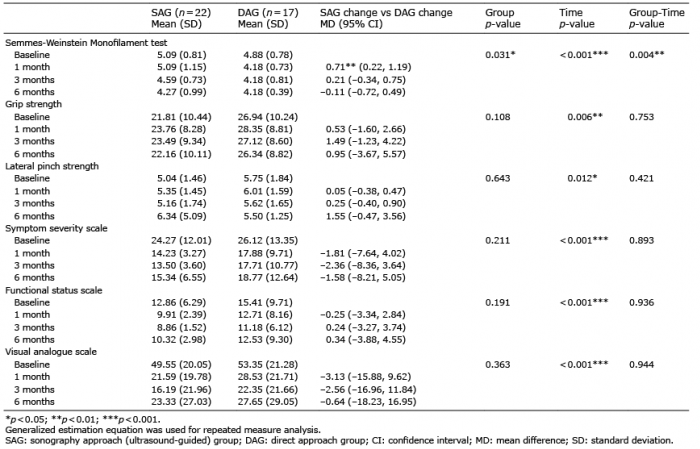 Click to show fullsize
Click to show fullsize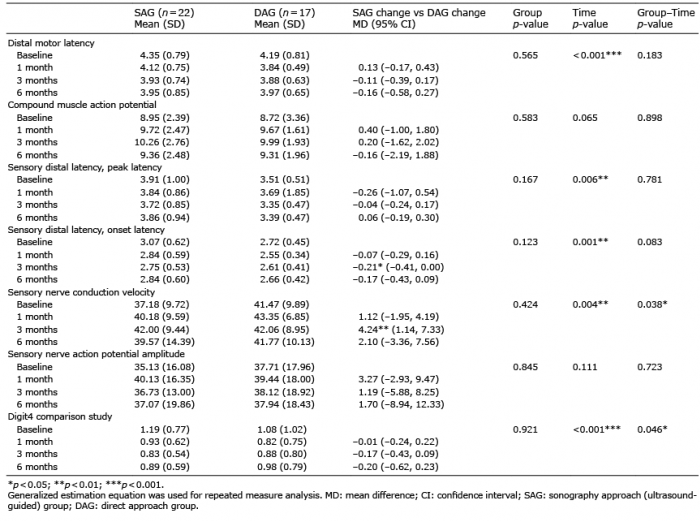 Click to show fullsize
Click to show fullsize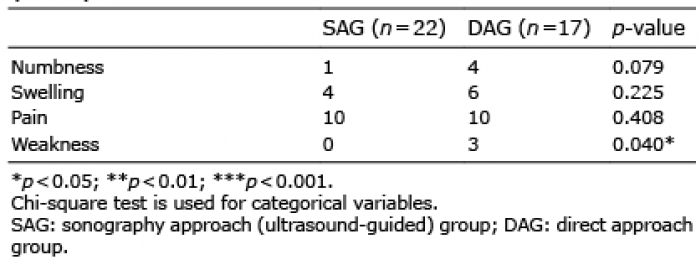 Click to show fullsize
Click to show fullsize